







Thomas Münzel, Andrea Pozzer and Jos Lelieveld from the Johannes Gutenberg University in Mainz, Germany examine the links between the pandemic and health.
An important observation during the COVID-19 pandemic was a huge reduction in the admission of patients with acute coronary syndrome to hospitals.
Importantly, similar was observed for patients with heart failure and arrhythmia such as atrial fibrillation.
There are several possibilities to explain this phenomenon, including the fear of contagion in hospitals or a substantial reduction in air pollution.
Indeed, during the first SARS pandemic, Cui et al. reported an ecologic study concerning air pollution and case fatality of SARS in the people republic of China.
With these studies, the authors found that there is a positive association between air pollution and SARS case fatality
in Chinese population and they calculated that in case of even a moderate air pollution index, infected patients had a
84% increased risk of dying from SARS 2.
Thus, a marked reduction of air pollution may indirectly indicate that air pollution has a significant effect on the incidence and outcome of patients with acute coronary syndrome.
COVID mortality and air pollution
The mortality of COVID-19 clearly depends on comorbidities including conditions such as cardiovascular risk factors such as diabetes mellitus, arterial hypertension, obesity and smoking.
Increased COVID-19 mortality is also associated with cardiovascular complications such as myocardial infarction, heart failure, arrhythmia and increases in biomarkers that are also found in connection with high levels of air pollutants.
Considering the cardiovascular and respiratory health impact of air pollution a relationship to COVID-19 mortality
is not very much surprising. Recently the severity of COVID-19 outcome was linked to PM2.5 µm exposure
in the USA.
With these studies, the authors established that the computed mortality rate ratios (MRRs), which express the relative increase in COVID-19 deaths for each microgram per cubic meter increment of PM2.5 in ambient air was found to be 11%.
Pozzer et al characterized the exposure to fine particles based on satellite data and calculated the anthropogenic fraction with an atmospheric chemistry model.The degree to which air pollution influences COVID-19 mortality was derived from epidemiological data in the USA and China. The authors estimated that air pollution contributed around 15% to COVID-19 mortality worldwide, 27% in East Asia, 19% in Europe and 17% in North America.
Globally 50-60% of the attributable anthropogenic fraction is related to fossil fuel use, up to 70-80% in Europe, West
Asia and North America.
The authors concluded that air pollution may represent an important risk of mortality from COVID-19.
Importantly, recent studies from Italy & England corroborate our findings of a significant link between air pollution and COVID-19.
Why does air pollution worsen the prognosis for patients with COVID-19 infections?
Air pollution is targeting the endothelium: Air pollution results from the complex interaction of multiple emissions and chemical reactions in the atmosphere, and the traditional classification of fine particles based on size or mass may provide an incomplete picture.
Over 70% of the fine particulate mass in the mixture in urban settings is from gases or vapour-phase compounds and secondary pollutants, including nitrogen dioxide (NO2), volatile organic compounds (including benzene), sulfur dioxide (SO2) and ammonia (NH3).
Combustion aerosols may contain coarse and ultrafine particles. While 10µm approximates the size of a cell, the ultrafine particles have the size of a virus. The smaller the particle the more likely it will penetrate the lung epithelium, enter the blood stream and is then taken up by the vessel wall.
Recent studies have indicated that worldwide around 8.8 Million excess deaths occur in response to air pollution (PM2.5 µm).
This translates into a reduction in life expectancy by 2.9 years while the cardiovascular risk factor tobacco smoking causes a reduction in life expectancy by 2.22 years pointing to the importance of ambient air pollution as a
cardiovascular risk factor.
Fine particulate matter PM2.5 has been demonstrated to increase oxidative stress within the vasculature, to reduce
nitric oxide, to increase inflammation, to increase oxidative stress and to cause endothelial (vascular) dysfunction 10.
These features caused by air pollution are strikingly parallel the ‘vascular pathology’ caused by the COVID-19 infection and may lead to cardiovascular diseases such a chronic coronary artery disease, acute coronary syndrome,
heart failure, thrombosis, pulmonary embolism as well as COPD and asthma.
This may explain at least in part why high levels of air pollution and thus an already damaged vasculature is more
susceptible to additional damage caused by the COVID-19 virus.
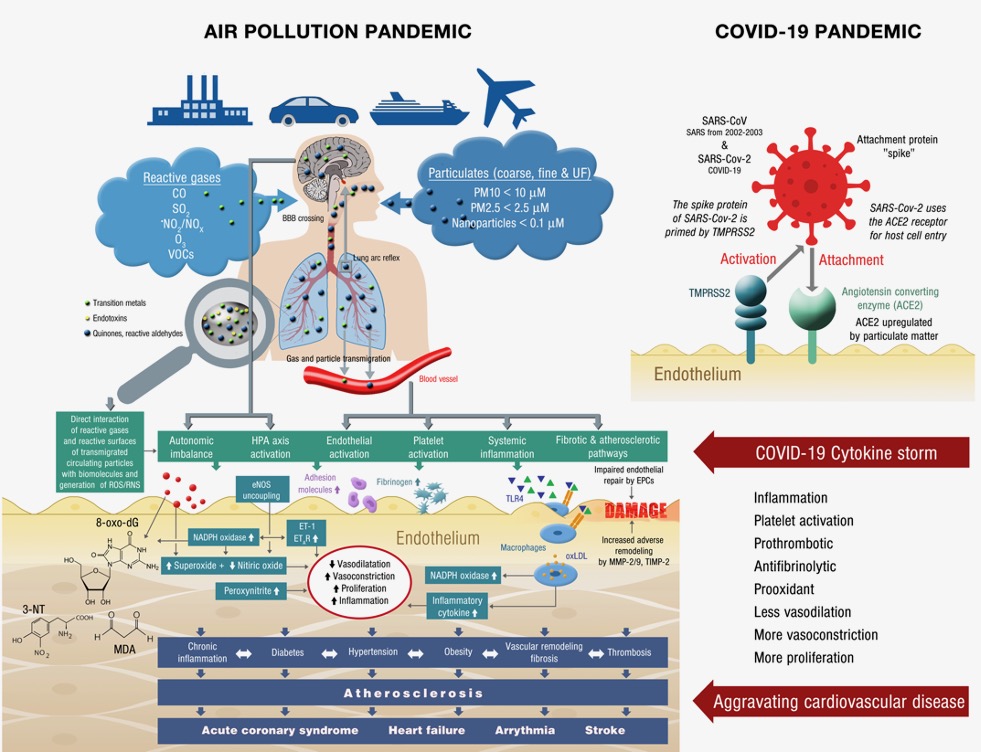
COVID-19 infection: in the end an endothelial disease too?
Lung injuries, respiratory failure as well as acute coronary syndrome, heart failure arrhythmia, thrombosis, pulmonary embolism and myocarditis have been shown to be critical complications of a COVID-19 infection.
With respect to the pathophysiology, Peter Libby and Tom Lüscher postulated in a recent review that COVID-19 may be at the end an endothelial disease.
The endothelium, which can be considered as a mechanical barrier between the bloodstream and tissues displays many features that regulate the vascular environment.
Thus, the endothelium strikingly participates on the regulation of the vasodilator/ vasoconstrictor balance, the balance between thrombosis and fibrinolysis and antioxidants/prooxidants and the inflammatory balance.
In case of a COVID-19 virus invasion, the endothelial cell is experiencing a so-called ‘cytokine storm’ that will stimulate the production of procoagulants such as tissue factor, thromboxane and the CD40 ligand, will act antifibrinolytic by inhibiting the formation of the plasminogen activator inhibitor (PAI-I), will decrease the endothelial nitric oxide production und increase the production of reactive oxygen species such as superoxide and peroxynitrite leading to endothelial dysfunction and thus to a procoagulant/prothrombotic milieu and subsequently to severe cardiovascular complications mainly myocardial infarction, acute heart failure, severe arrhythmia
or myocarditis
Conclusions and clinical implications
The results of the presented studies suggest the potential for substantial benefits from reducing air pollution exposure even at relatively low PM2.5 levels.
Refinement of the exposure-response relationship and reducing uncertainties will require additional data analyses, including from large cohort studies as the COVID-19 pandemic evolves, but may appear too late to guide decision-making.
A lesson from our environmental perspective of the COVID-19 pandemic is that the quest for effective policies to reduce anthropogenic emissions, which cause both air pollution and climate change, needs to be accelerated.
The pandemic ends with the vaccination of the population or with herd immunity through extensive infection of the population.
However, there are no vaccines against poor air quality and climate change.
The remedy is to mitigate emissions. The transition to a green economy with clean, renewable energy sources will further both environmental and public health locally through improved air quality and globally by limiting climate change.